Why Do We Miss Stuff?
Brace yourself. I miss stuff.
Whew! It almost feels better now that I’ve written it down. It’s harder to admit than you think. I’d like to think I’m the greatest radiologist on the planet, but there can only be one of those, and he’s somewhere in Texas. So, I guess I have to make due with the skills I have and try to decrease my misses – both in numbers and egregiousness.
But how? Sure, the retrospectoscope can highlight mistakes. It’s painful when the surgeon comes to you with a black colon in a jar and says, “Would you mind reviewing the CT again?” You go back and say, “damn.” You justify. You make excuses. “I was extra busy that day. There were a lot of distractions.” And so on, and so forth…
I like to confront my inadequacies head-on, so I got myself appointed as Chief of QA at a major medical center. It’s a mixed blessing. On the one hand, I get to point out every else’s mistakes, which fits real well with my need to feel superior. On the other hand, my own misses have not escaped the conference, and I’m harder on myself then anyone else.
Now that I’ve been doing this a while, I’ve started noticing trends. I’m sure none of this is new information, but I think it helps to hear it now and then. Here is what I tell my residents and fellow staff.
There are two well known ways to make a mistake in radiology:
1. Failure to see the pertinent findings.
2. Failure to synthesize what the findings mean.
 Figure 1. This case was read as “Normal chest.”
Figure 1. This case was read as “Normal chest.”
 Figure 2. Not normal.
Figure 2. Not normal.
If you’ve done this job for more than one or two days, you are probably guilty of both types of mistakes. Certainly, we all made these mistakes with some frequency in residency. Hopefully, the errors are fewer and further between now that we have graduated.
Now I’d like to propose a third category of mistakes, which may in fact be a subset of #2:
3. Lack of intellectual curiosity.
This is a tough one. Many things can influence your natural curiosity. How many exams did you read that day? Were there unusual distractions? When you see something you don’t understand, do you stop and look it up? Do you take the time to query your database for additional lab findings and biopsy results? Do you call your CT surgeon when you see a new type of coronary artery stent? What textbooks sit beside your reading station? What websites do you have bookmarked?
Passing boards means that we have been deemed safe, but is that enough? A periodic hard and truthful look in the mirror and an honest assessment of our shortfalls can make a difference. It won’t change your mistakes - those have already happened. What you hope is that your NEXT patient will benefit.
Brace yourself. I miss stuff.
Whew! It almost feels better now that I’ve written it down. It’s harder to admit than you think. I’d like to think I’m the greatest radiologist on the planet, but there can only be one of those, and he’s somewhere in Texas. So, I guess I have to make due with the skills I have and try to decrease my misses – both in numbers and egregiousness.
But how? Sure, the retrospectoscope can highlight mistakes. It’s painful when the surgeon comes to you with a black colon in a jar and says, “Would you mind reviewing the CT again?” You go back and say, “damn.” You justify. You make excuses. “I was extra busy that day. There were a lot of distractions.” And so on, and so forth…
I like to confront my inadequacies head-on, so I got myself appointed as Chief of QA at a major medical center. It’s a mixed blessing. On the one hand, I get to point out every else’s mistakes, which fits real well with my need to feel superior. On the other hand, my own misses have not escaped the conference, and I’m harder on myself then anyone else.
Now that I’ve been doing this a while, I’ve started noticing trends. I’m sure none of this is new information, but I think it helps to hear it now and then. Here is what I tell my residents and fellow staff.
There are two well known ways to make a mistake in radiology:
1. Failure to see the pertinent findings.
2. Failure to synthesize what the findings mean.
 Figure 1. This case was read as “Normal chest.”
Figure 1. This case was read as “Normal chest.”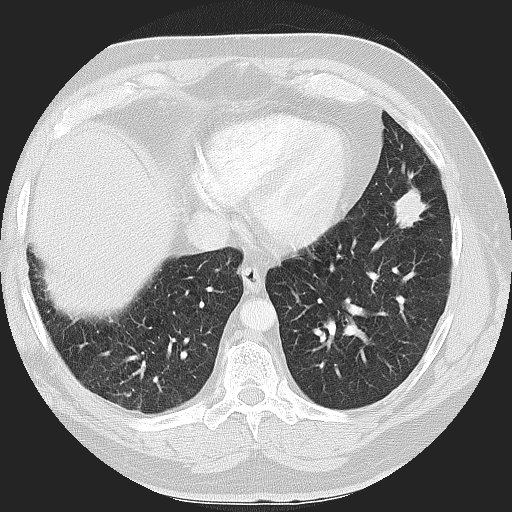 Figure 2. Not normal.
Figure 2. Not normal.If you’ve done this job for more than one or two days, you are probably guilty of both types of mistakes. Certainly, we all made these mistakes with some frequency in residency. Hopefully, the errors are fewer and further between now that we have graduated.
Now I’d like to propose a third category of mistakes, which may in fact be a subset of #2:
3. Lack of intellectual curiosity.
This is a tough one. Many things can influence your natural curiosity. How many exams did you read that day? Were there unusual distractions? When you see something you don’t understand, do you stop and look it up? Do you take the time to query your database for additional lab findings and biopsy results? Do you call your CT surgeon when you see a new type of coronary artery stent? What textbooks sit beside your reading station? What websites do you have bookmarked?
Passing boards means that we have been deemed safe, but is that enough? A periodic hard and truthful look in the mirror and an honest assessment of our shortfalls can make a difference. It won’t change your mistakes - those have already happened. What you hope is that your NEXT patient will benefit.
posted by DrChako at
10:03 AM
![]()
![]()


1 Comments:
As an aside, this case was not mine, but I'm capable of this kind of miss, as are most radiologists, I think.
Post a Comment
Subscribe to Post Comments [Atom]
<< Home